Cauliflower Ear
Cauliflower Ear (a.k.a. Auricular Hematoma)
Next to skin infections, nothing affects wrestlers more than cauliflower ear. Since the beginning of this sport, ear trauma has been well documented. It develops due to ear trauma causing a separation of the perichondrium covering the auricular cartilage. Once separated the space fills with blood and if left alone will harden causing the thickening or abnormal pattern similar to a head of cauliflower.
Statistics show that the use of headgear helps to reduce its development. Devised many decades ago, but not required by the NCAA until the late 1960s, headgear has become much more comfortable and conforming to the head.
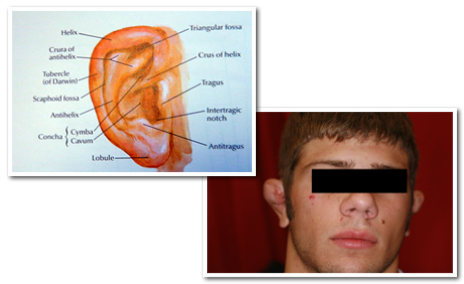
Even so, its usage varies and statistics show that amongst Div 1 NCAA wrestlers, 35.2% will wear it during practice. Contrast that with 92.4% during competition. Obviously, since this study in 1989, the rate of usage during competition is higher than that (Actually it is required during all competition). But the obvious fact is that almost 2/3’s of wrestlers don’t wear them during practice and this is reflective in that the majority of cauliflower ear development occurs with the headgear off (79% based on coach’s observation). To understand its development, it’s important to have a general understanding of the body parts involved. The ear is a simple structure that serves to funnel in sound and aid in hearing.
Even so, its usage varies and statistics show that amongst Div 1 NCAA wrestlers, 35.2% will wear it during practice. Contrast that with 92.4% during competition. Obviously, since this study in 1989, the rate of usage during competition is higher than that (Actually it is required during all competition). But the obvious fact is that almost 2/3’s of wrestlers don’t wear them during practice and this is reflective in that the majority of cauliflower ear development occurs with the headgear off (79% based on coach’s observation). To understand its development, it’s important to have a general understanding of the body parts involved. The ear is a simple structure that serves to funnel in sound and aid in hearing.

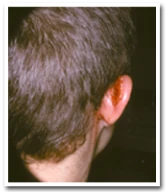
Acute auricular hematoma
Acute auricular hematoma
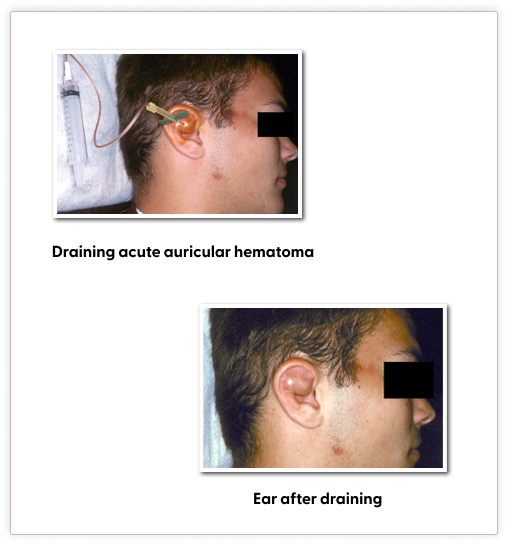
On average, it takes about 7-10 days after blood develops in this space for it to start to harden. If removed before that time, or while the fluid is still liquid, cauliflower formation can be prevented. Once it is hard, removal becomes more difficult and usually requires surgical intervention. Removal of fluid can be performed in several ways. Acute or recent injuries are the easiest. Injuries that are several days old are more difficult. Remember, perichondrial formation of cartilage develops over 7-10 days, so as time goes on this blood gets thicker with new cartilage formation called neofibrocartilage. As this material develops it causes the fluid to get thickened. So fresh injuries are amenable via aspiration of the blood via a small needle.
But older pockets of fluid have thickened due to neofibrocartilage, thus making them more difficult to drain, or aspirate. Usually, a larger needle or even cutting open the area is necessary to remove the material. Once the blood has been removed the most important means to prevent recurrence is – compression! Regardless of how well the aspiration went, if you don’t compress the site, blood will reaccumulate and blowback up to the same size. This is where Health Care Providers are confused and ignorant of this sport. Compression can be obtained via various means, but each method has its advantages and disadvantages. Over the past several decades’ various means have developed to apply compression to the ear.
But older pockets of fluid have thickened due to neofibrocartilage, thus making them more difficult to drain, or aspirate. Usually, a larger needle or even cutting open the area is necessary to remove the material. Once the blood has been removed the most important means to prevent recurrence is – compression! Regardless of how well the aspiration went, if you don’t compress the site, blood will reaccumulate and blowback up to the same size. This is where Health Care Providers are confused and ignorant of this sport. Compression can be obtained via various means, but each method has its advantages and disadvantages. Over the past several decades’ various means have developed to apply compression to the ear.
What usually makes this difficult is that it takes 6 weeks for the perichondrium to adequately knit down and adhere to the cartilage surface, but none of these procedures are meant to be in place that long. Therefore unless the athlete is at the end of his season or is willing to sit out for 6 weeks, some blood will reaccumulate back into the site and harden. Below is a list of procedures to treat cauliflower ear with the advantages and disadvantages. Description of each procedure will be given later on in the article.
Means to Compress after draining Auricular Hematoma
Simple Wrap
Pros:
- Quick and simple
- Can continue to wrestle
Cons:
- Poor compression
- Poor compliance
Dental caulking
Pros:
- Quick and simple
- Good compression
- Fairly good results
Cons:
- Cost of equipment
- Can’t continue to wrestle with it
Thermoplastic splint
Pros:
- Excellent results
- Excellent compression
- Can continue to wrestle
Cons:
- Office-based surgical procedure
- Increased risk of infection
Magnets
Pros:
- Easily accessible
- Easily applied
Cons:
- Can’t be used while wrestling
- Poor compliance by users leads to blood reaccumulating
With progress, new means to treat this condition develop. With the newer materials available, it is this author’s opinion that collodion casts and dental cotton roll bolsters should no longer be used to treat this condition. Collodion contains ether- a very flammable substance that takes up to 30-40 minutes to apply.
Cotton roll bolsters sutured as means to compress the ear increases the risk for infection via collecting bacteria.
Cotton roll bolsters sutured as means to compress the ear increases the risk for infection via collecting bacteria.

Compression Procedures:

Wrapping- After draining the hematoma, apply gauze to the front and back of the ear then wrap it with a roll of Coban®. This compression should be kept in place 24/7 for the next 2 weeks. Removal after each practice, ice the ear down for 10 minutes then shower. Rewrap after showering. Make sure the headgear fits over this wrap during practice.
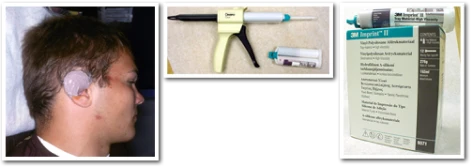
Dental caulking- This material requires purchasing Dentsply® dental gun and silastic material. After draining the ear, it is applied to the ear to the front and back. It will harden in 5 minutes. Don’t cover the ear canal. The idea here is to form a ‘clam shell’ over the ear to compress it and reduce the reaccumulation of blood in the pocket. This is the best means to treat an ear at the end of the season. Keep in place for 3 days, then remove. Peels off like a mouthguard. Ice the area for 10 minutes 3-4 times a day for the next 1 week.
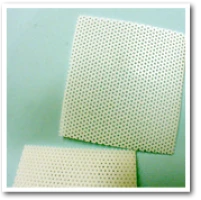
Thermoplastic splint- After draining the ear, prep the area in a sterile fashion. Consider local anesthesia with 1% lidocaine. Using a piece of 1/16” Aquaplast®, cut an outline of the front of the ear with the material, where the hematoma was drained. Using boiling water, warm the piece and conform it to the area of concern. The same was done to the back of the ear. Let the material slightly cool before applying it to the ear to form it. Once the 2 pieces are formed, a piece of Adaptic® (vaseline coated gauze) was fitted to each piece then applied to the front and back of the ear. At this time the ear is sandwiched between each of these pieces and sutured in place with two loops of 3.0 nylon suture. Afterward, gauze is placed in the front and back of the ear then wrapped with Coban®. Keep in place for 24 hours and no wrestling during this period. After 24 hours the Coban® wrap can be removed. Rewrap with gauze in front and back for practice. Make sure the headgear can fit over the wrap. After practice, remove the Coban® and gauze. Ice the area for 10 minutes and shower. Cleanse the area with hydrogen peroxide and apply a topical antibiotic to the area. Leave open to the air. Can shower with the splint in place. No swimming, hot tub, or submersion in the tub until 24 hours after removal of the splint. A splint can be removed in 2 weeks.
Also, place wrestler on oral antibiotics to cover for staph and strep for the first week.

Conclusion:
Remember, drain the area as soon as possible. Application of pressure is necessary or blood will reaccumulate into the space. Finally try to leave the ear alone. The longer you can stay away from wrestling, the better the result will be. Any return too soon compromises the result and runs the risk for blood to reaccumulate. Once the area is hard, then surgical revision by a specialist will be the only way to correct the problem.
Summary:
1. Drain
2. Pressure
3. Don’t putz with it!
References:
Schuller DE, Dankle SK, Martin M, Strauss RH. Auricular Injury and the use of Headgear in Wrestlers. Arch Otolaryngol Head Neck Surg. 1989;115:714-17.
Giffin CS. Wrestler’s Ear: Pathology and Treatment. Annals of Plastic Surg. 1992;28(2):131-39.
Henderson JM, Salama AR, Blanchaert RH. Management of Auricular Hematoma Using a Thermoplastic Splint. Arch Otolaryngol Head Neck Surg. 2000;126:888-890.
Giffin CS. Wrestler’s Ear: Pathology and Treatment. Annals of Plastic Surg. 1992;28(2):131-39.
Henderson JM, Salama AR, Blanchaert RH. Management of Auricular Hematoma Using a Thermoplastic Splint. Arch Otolaryngol Head Neck Surg. 2000;126:888-890.
Medical Disclaimer
The above procedures reflect information gathered by medical professionals who are trained and licensed in the medical profession. Under no circumstances does this information serve as a guide for the lay public to perform these procedures. Any individual who performs these procedures does so at his or her risk. The Mat Doc, LLC takes no responsibility for anyone performing these procedures and having a complication or unsatisfactory outcome. The above-mentioned materials are used in an unapproved fashion by their makers: Dentsply, 3M Co, Johnson and Johnson, the makers of Coban adhesive wrap, and Adaptic vaseline gauze. Anyone using these materials outlined above does so at his or her own risk.